How to Get Rid of a Chronic Cough: Causes, Remedies, and Treatment Options
A cough that lasts for weeks can be exhausting—especially when it disrupts sleep, strains your voice, or makes everyday conversations uncomfortable. Many chronic coughs improve when the underlying cause is identified and treated, rather than relying only on cough suppressants. Contemporary guidance emphasizes this targeted approach because the most common drivers are often treatable. (Mayo Clinic, 2024; British Thoracic Society, 2024)
Think of chronic cough like a smoke alarm that keeps chirping. A suppressant might quiet it briefly, but the lasting fix is finding what’s setting it off—upper airway cough syndrome (often related to postnasal drip), asthma-related airway inflammation, reflux, medication side effects, or an overly sensitive cough reflex.
Medical note: This article is educational and not a substitute for personalized medical care. If you have severe symptoms or red flags (below), seek urgent evaluation.
What Counts as a Chronic Cough (and Why It Matters)
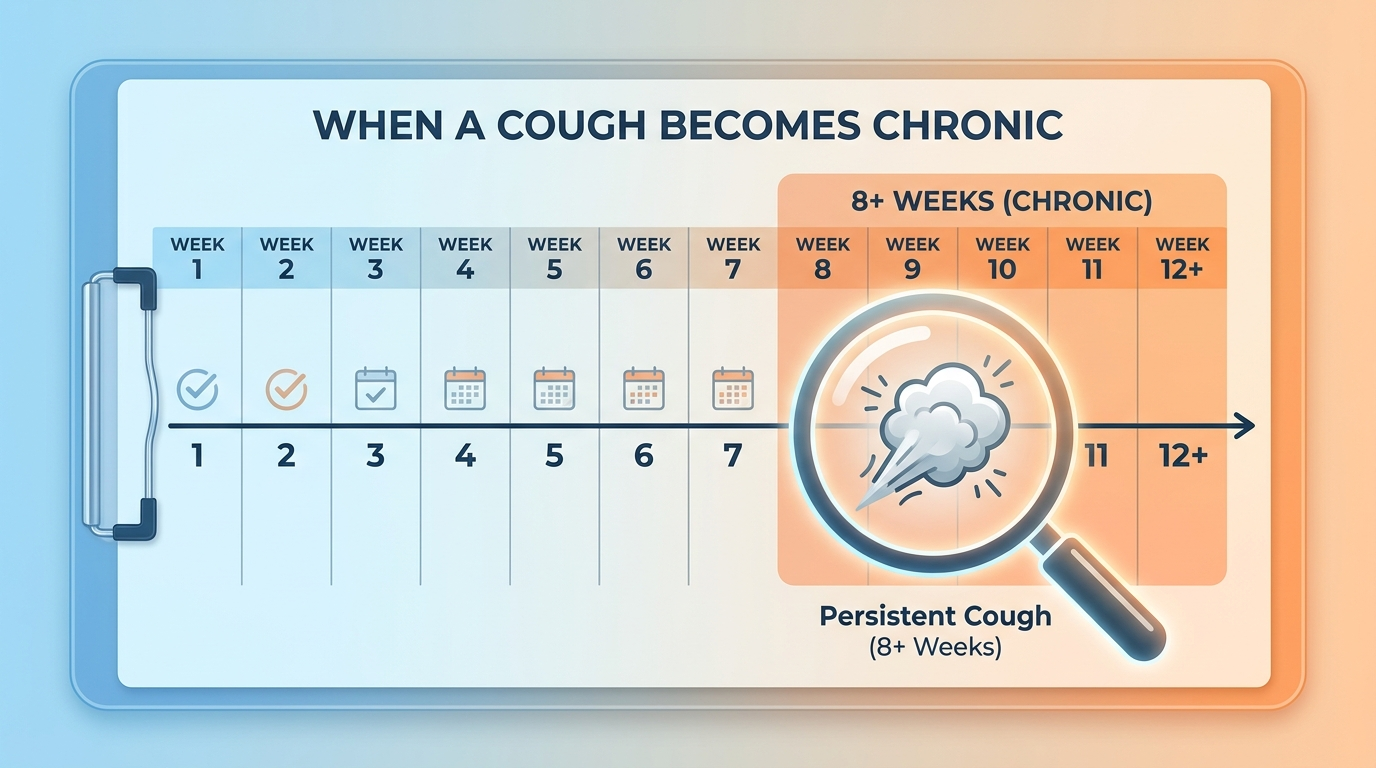
In adults, a cough is generally considered chronic if it lasts 8 weeks or longer. In children, cough lasting more than 4 weeks is often considered chronic and may need earlier evaluation. (Mayo Clinic, 2024)
Why not just wait it out? Because ongoing coughing can:
- Signal a treatable issue such as cough related to postnasal drip (upper airway cough syndrome), GERD-related cough, or cough-variant asthma
- Lead to throat irritation, hoarseness, poor sleep, and reduced quality of life
- Occasionally point to something more serious that shouldn’t be missed (Mayo Clinic, 2024)
A common approach is to identify the underlying cause and match treatment to it, rather than suppressing the symptom alone.
In short: defining chronic cough (8+ weeks in adults; 4+ weeks in children) helps you get to targeted, more effective care.
Chronic Cough Symptoms to Pay Attention To
Common ways a chronic cough feels:
- Dry (no mucus) or productive (mucus/phlegm)
- Worse at night, after meals, with exercise, or when lying down
- Associated with a throat tickle, irritation, or frequent throat clearing (sometimes linked to cough hypersensitivity)
- Paired with hoarseness/voice strain and disrupted sleep
A common story clinicians hear is: “I’m fine during the day, but the moment I lie down, I start coughing.” That pattern can be a clue—often pointing toward upper-airway drainage or reflux-related triggers.
Red flags—get urgent medical care if you have:
- Coughing up blood, unexplained weight loss, or persistent fever
- Shortness of breath, chest pain, or wheezing that is new or severe
- Recurrent pneumonia, choking episodes, or symptoms that persist despite evaluation (Mayo Clinic, 2024)
Key takeaway: track patterns and watch for red flags—these details help guide safer, faster diagnosis.

The “Treatable Traits” Approach—Why Treating the Cause Works Better Than Suppressing the Cough
Newer guidance often describes a “treatable traits” strategy: look for specific, common drivers and treat them directly. Many over-the-counter products (and even some prescription options used without a clear diagnosis) don’t help much if the true cause is reflux, asthma-related airway inflammation, or upper-airway drainage. (British Thoracic Society, 2024; Mayo Clinic, 2024)
A practical way to apply this at home is to notice timing and triggers:
- Meals and bending over can hint at reflux.
- Nighttime and exercise can align with asthma patterns.
- Morning cough and throat clearing can fit cough related to postnasal drip.
Bottom line: identifying what triggers your cough reflex guides treatment that works better and lasts longer.
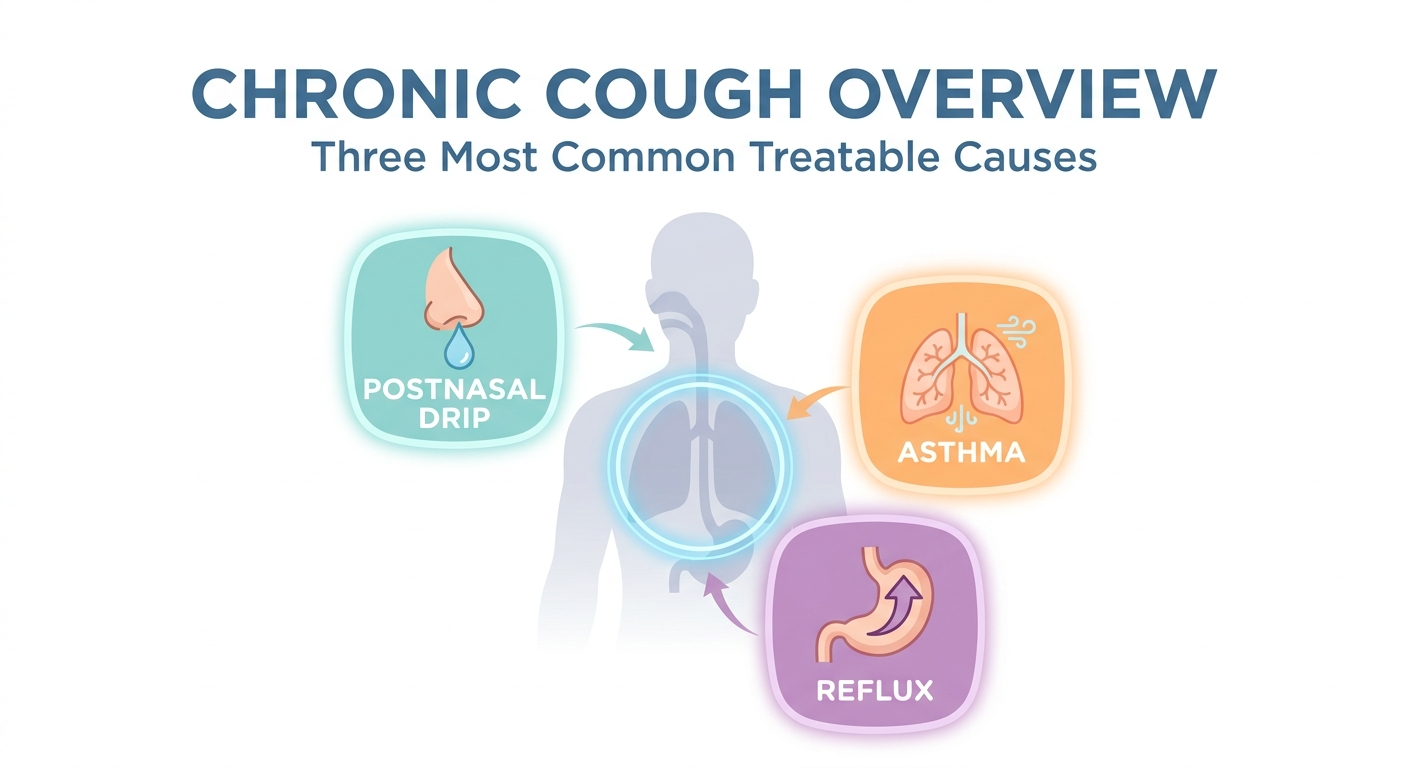
Three Common Causes of Chronic Cough in Adults (and What to Do)
Among adults, upper airway cough syndrome (often related to postnasal drip), asthma (including cough-variant asthma), and GERD are among the most common causes of chronic cough. (Mayo Clinic, 2024; British Thoracic Society, 2024)
Cause #1 — Postnasal Drip (Upper Airway Cough Syndrome)
Clues it may be postnasal drip:
- Feeling mucus in the throat, frequent throat clearing, nasal congestion
- Cough worse when lying down or first thing in the morning
Some people describe it as a drip they can’t swallow away—leading to repeated throat clearing that keeps the throat irritated.
Targeted treatments (often first-line):
- Intranasal steroid sprays used consistently (not just as needed)
- Saline rinses/irrigation (with safe technique)
- Identifying triggers such as allergies, chronic rhinitis, or sinus inflammation (Mayo Clinic, 2024; British Thoracic Society, 2024)
For a deeper dive on ENT-focused options, see Sleep and Sinus Centers of Georgia’s guide on ENT treatments for chronic postnasal drip: https://sleepandsinuscenters.com/blog/chronic-post-nasal-drip-ent-treatments-that-work
Summary: treating nasal and sinus inflammation directly can quiet the drip—and the cough it triggers.

Cause #2 — Asthma (Including Cough-Variant Asthma)
Clues it may be asthma:
- Wheeze, chest tightness, shortness of breath
- Cough with exercise, cold air, or at night
- A cough-only pattern known as cough-variant asthma
Even if you don’t feel overtly wheezy, a cough that shows up with runs, cold air, or laughter can still fit an asthma-type pattern.
Targeted treatments:
- Inhaled corticosteroids (controller therapy) to reduce airway inflammation
- Trigger control and an asthma action plan, when appropriate (Mayo Clinic, 2024; British Thoracic Society, 2024)
Takeaway: consistent controller therapy often helps most for asthma-related cough.

Cause #3 — GERD (Acid Reflux) or LPR (“Silent Reflux”)
Clues it may be reflux-related:
- Heartburn, sour taste, cough after meals
- Throat clearing, hoarseness, or a lump in throat sensation—sometimes even without heartburn
Silent reflux is a lay term for laryngopharyngeal reflux (LPR), which can irritate the throat and trigger cough even when classic heartburn is absent. Sleep and Sinus Centers of Georgia explains more here: https://sleepandsinuscenters.com/blog/silent-acid-reflux-and-chronic-cough-understanding-the-link
Targeted treatments:
- Lifestyle changes (meal timing, sleep position, identifying trigger foods)
- Proton pump inhibitors (PPIs) may be considered when reflux is suspected, ideally under clinician guidance, with reassessment if symptoms do not improve (Mayo Clinic, 2024; British Thoracic Society, 2024)
In brief: when reflux is suspected, timing of symptoms around meals and lying down helps guide next steps.

Other Common (and Often Missed) Causes of Chronic Cough
ACE inhibitor medications (blood pressure meds): ACE inhibitors are a well-known cause of a dry, persistent cough in some people. Medication changes should be discussed with the prescribing clinician rather than stopping on your own. (Mayo Clinic, 2024)
Smoking and vaping: Smoking and vaping can cause chronic airway irritation and inflammation. Quitting can be one of the most impactful steps for long-term respiratory health, though some people notice temporary cough sensitivity during nicotine withdrawal. (Mayo Clinic, 2024; British Thoracic Society, 2024)
Infections and post-viral cough: A cough can linger after a respiratory infection. If it crosses the 8-week mark in adults, it often warrants a structured evaluation for other treatable causes rather than assuming it will fade on its own. (Mayo Clinic, 2024)
Less common but important causes (brief list):
- Chronic bronchitis/COPD, bronchiectasis
- Lung disease, tumors, heart failure (less common, but important)
- Environmental/occupational irritants (dust, fumes, strong scents)
Essentials: if a cough persists, consider medications, exposures, and less common conditions—especially if red flags are present.
Step-by-Step: How Doctors Diagnose a Chronic Cough
What to expect at a medical evaluation:
- History: timing, patterns, triggers (meals, lying down, exercise), medication list (including ACE inhibitors), smoking/vaping, and exposures
- Physical exam: nose/throat/chest focus
Bringing a short cough timeline can help: when it started, what makes it worse, what you’ve tried, and whether you’re bringing up mucus.
Common tests used to rule in treatable causes:
- Chest X-ray (often early, to look for concerning causes)
- Spirometry (lung function testing) to assess asthma/COPD patterns
- FeNO testing, where available, may help identify eosinophilic airway inflammation that can support an asthma-related diagnosis (Mayo Clinic, 2024; British Thoracic Society, 2024)
Why trial-and-error cough syrup often falls short: If the cough is driven by reflux, airway inflammation, or upper-airway drainage, a generic suppressant may offer only limited benefit—because it doesn’t address the driver. (British Thoracic Society, 2024)
Practical point: targeted evaluation and testing help match the treatment to the cause—and save time.
Evidence-Based Treatments to Get Rid of a Chronic Cough (By Cause)
Treatment plan for postnasal drip–related cough
Common components include:
- Daily nasal steroid with correct technique and enough time to see effect (often weeks, not days)
- Saline irrigation routines and trigger reduction (smoke, fragrances, dusty environments)
- Considering allergy evaluation or ENT assessment when symptoms persist or sinus disease is suspected (Mayo Clinic, 2024; British Thoracic Society, 2024)
For practical tips, see how to use a steroid nasal spray correctly: https://sleepandsinuscenters.com/blog/steroid-nasal-spray-technique-step-by-step-guide-for-effective-use
Short version: consistent, correct nasal therapy often reduces drip—and the cough that follows.
Treatment plan for asthma/cough-variant asthma
Education often focuses on:
- Why inhaled corticosteroids work best when taken consistently (they reduce inflammation over time)
- The difference between a rescue inhaler (quick relief) and a controller inhaler (prevention)
- Symptom tracking and follow-up testing (like spirometry) when recommended (Mayo Clinic, 2024; British Thoracic Society, 2024)
A helpful mindset: controllers are maintenance—benefits build with steady use.
Treatment plan for GERD/LPR cough
Foundational strategies often include:
- Meal timing (avoiding late meals) and smaller portions
- Sleep positioning strategies (such as head-of-bed elevation)
- Medication trials (like PPIs) in selected cases, with a plan to reassess response (Mayo Clinic, 2024; British Thoracic Society, 2024)
Tip: aligning treatment with symptom timing—after meals, with bending, or overnight—improves the odds of success.
When the Cough Won’t Go Away: Cough Hypersensitivity (Nerve-Driven Cough)
Sometimes triggers have been treated, but coughing persists because the cough reflex has become overly sensitive—often called cough hypersensitivity. Common triggers include:
- Talking or laughing
- Cold air
- Perfumes/strong smells
- A persistent throat tickle
You can think of this as the volume knob on the cough reflex being turned up too high—so small triggers set it off.
Medications sometimes used for refractory chronic cough (specialist-directed): In select refractory cases, specialists may consider treatments such as gabapentin or, less commonly, low-dose morphine under careful supervision. (British Thoracic Society, 2024)
Non-medication therapy that can help: Speech and Language Therapy (SLT) / cough control therapy can teach breathing strategies, swallow techniques, and cough-suppression tools that reduce the urge to cough. (British Thoracic Society, 2024)
For next-step options, see ENT procedures that can help with chronic cough: https://sleepandsinuscenters.com/blog/ent-procedures-that-help-with-chronic-cough
Bottom line: when sensitivity is the driver, behavioral therapy—and sometimes specialist medications—can turn the volume down.
Lifestyle Tips That Can Reduce Chronic Cough Triggers (Even While You’re Getting Diagnosed)
Home and environment:
- Avoid smoke exposure; consider quitting smoking/vaping if relevant
- Improve indoor air quality: ventilation, HEPA filtration if helpful, and reducing irritant fragrances/cleaners
- Hydration and (in some homes/climates) thoughtful humidification may reduce throat irritation
Daily habits:
- Track patterns: after meals, nighttime, exercise, seasonal changes—this can help pinpoint likely causes
- Voice care: frequent throat clearing can perpetuate irritation; sipping water or using a gentle swallow may help
Think of these as background reducers while you and your clinician identify the main driver.
FAQs About Chronic Cough
Why does my chronic cough get worse at night?
Nighttime worsening commonly aligns with postnasal drip pooling when lying down, reflux that’s worse when horizontal, or asthma patterns that flare overnight. (Mayo Clinic, 2024; British Thoracic Society, 2024)
Can allergies cause a chronic cough?
Yes. Allergies often contribute through upper airway cough syndrome/postnasal drip. Testing and targeted treatment may help when allergies are suspected. (Mayo Clinic, 2024)
What’s the fastest way to stop a chronic cough?
Fast depends on the cause. The most effective approach is typically targeted therapy—treating cough related to postnasal drip, asthma-related airway inflammation, or reflux—rather than relying only on suppressants. (British Thoracic Society, 2024)
Should I use OTC cough medicine?
OTC products may offer short-term comfort for some people, but they often don’t resolve chronic cough if the underlying driver isn’t addressed. (British Thoracic Society, 2024)
When should I see a doctor for a cough?
Consider evaluation if it lasts 8+ weeks (adults), disrupts sleep/work, or includes red flags like coughing up blood, chest pain, or shortness of breath. (Mayo Clinic, 2024)
Remember: matching the treatment to the cause is the key to lasting relief.
Conclusion — A Practical Next-Step Plan
1. Confirm it’s chronic (8+ weeks in adults; 4+ weeks in children) and screen for red flags.
2. Review common drivers: upper airway cough syndrome (postnasal drip), asthma (including cough-variant asthma), and reflux—plus medication triggers like ACE inhibitors.
3. Seek a structured evaluation, which often includes a chest X-ray and spirometry (and sometimes FeNO as supportive testing).
4. If coughing persists despite appropriate treatment, ask about cough hypersensitivity and options like cough control therapy/SLT. (Mayo Clinic, 2024; British Thoracic Society, 2024)
If you’d like help pinpointing what’s driving your symptoms—especially if postnasal drip, reflux, or upper-airway irritation seems likely—you can book an appointment with Sleep and Sinus Centers of Georgia: https://www.sleepandsinuscenters.com/
Next step: partner with a clinician to match treatment to your cough’s true cause.
References
Mayo Clinic. (2024). Chronic cough: Symptoms and causes. https://www.mayoclinic.org/diseases-conditions/chronic-cough/symptoms-causes/syc-20351575
British Thoracic Society. (2024). Clinical Statement: Chronic Cough (referenced via Medscape summary). https://reference.medscape.com/cc2/p10/british-thoracic-society-clinical-statement-chronic-cough-2024a10008ag
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
Don’t let allergies slow you down. Schedule a comprehensive ENT and allergy evaluation at Sleep and Sinus Centers of Georgia. We’re here to find your triggers and guide you toward lasting relief.