Septoplasty and Sinus Surgery: When ENT Specialists Recommend Combining Procedures
Quick Take—Why ENTs Sometimes Combine Septoplasty + Sinus Surgery
If you have both a deviated septum (which can block nasal breathing) and chronic rhinosinusitis (CRS)—longstanding sinus inflammation with pressure, drainage, or recurrent symptoms—an ENT may recommend septoplasty and sinus surgery in the same operation. The goal is straightforward: address structural blockage and sinus drainage problems together—often in a single operative session with one recovery period.
Many patients describe it like this: “My nose feels blocked all the time, and I’m also constantly dealing with sinus pressure or drainage.” When both issues are present, fixing only one can leave you with leftover symptoms. Published studies suggest combined surgery can be safe and effective in appropriately selected patients. [1–3]
—
Big picture: when structural blockage and chronic inflammation coexist, treating both in one planned session can be efficient and symptom-focused.
Understanding the Two Procedures (and What Each One Fixes)
What Septoplasty Treats
Septoplasty is surgery to straighten the nasal septum—the wall of cartilage and bone between the nostrils. When the septum is significantly off-center, it can narrow one side of the nose and contribute to nasal obstruction (blocked nasal breathing). Some people notice it most at night or during exercise; others feel it constantly.
What septoplasty may improve:
- Day-to-day ability to breathe through the nose
- Reduced reliance on mouth-breathing (especially at night) when blockage is a major factor
- Improved nasal airflow that can make other nasal/sinus treatments work better
A simple way to think about it: septoplasty helps “open the main hallway” so air can move more freely.
If you’re learning the basics of a deviated septum and common symptoms, see our education page on deviated septum relief: https://sleepandsinuscenters.com/deviated-septum-relief

What Functional Endoscopic Sinus Surgery (FESS) Treats
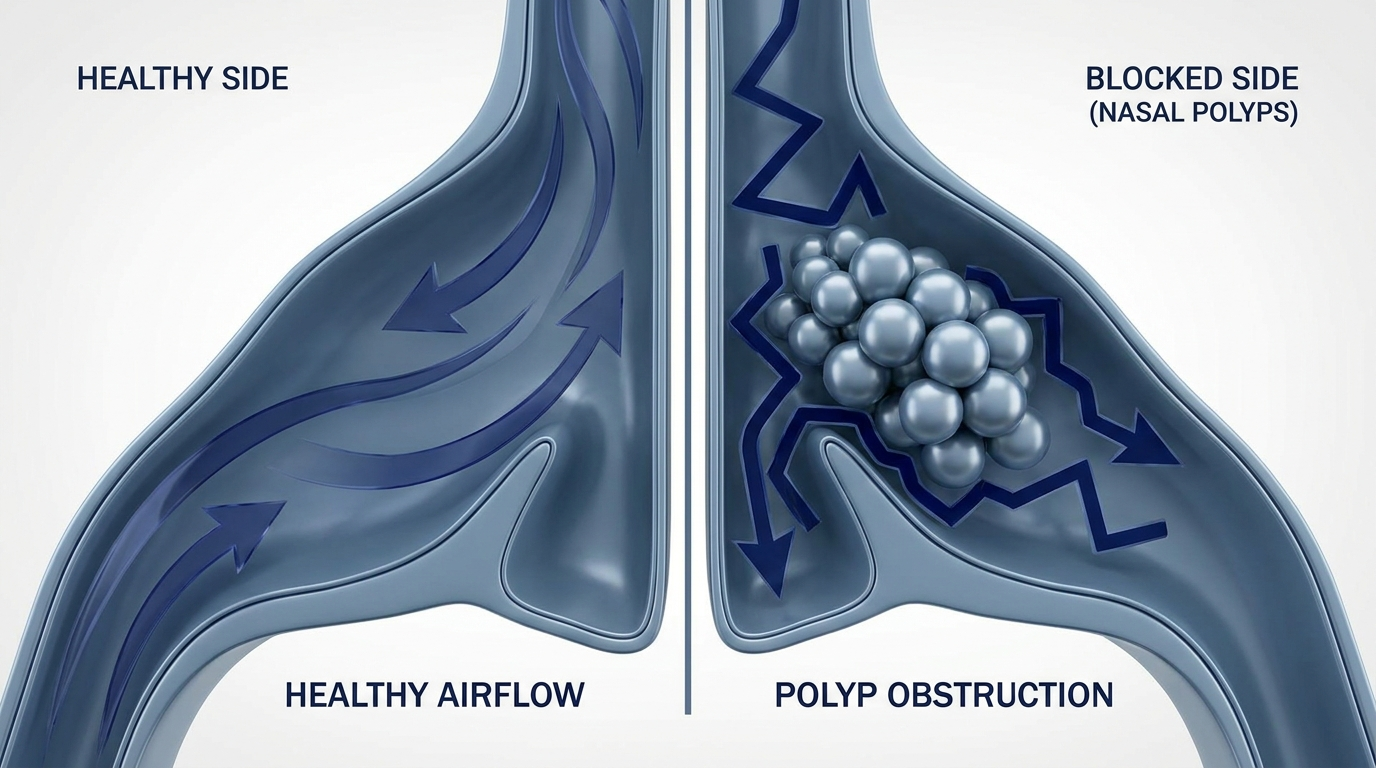
Functional endoscopic sinus surgery (FESS) is a minimally invasive technique that uses small cameras and instruments to open blocked sinus drainage pathways and address ongoing inflammation (and sometimes polyps). The aim is to help the sinuses ventilate and drain more normally—so mucus doesn’t get “stuck,” and topical medications can reach the right areas more effectively after healing.
Typical goals of FESS:
- Fewer chronic sinus symptoms and inflammation flares over time
- Less facial pressure/fullness related to blocked drainage
- Improved mucus clearance and reduced postnasal drip (for many patients)
- Better access for topical treatments (like saline or medicated sprays/rinses) after healing [3–4]
For a patient-friendly overview, you can also read our endoscopic sinus surgery guide: https://sleepandsinuscenters.com/blog/endoscopic-sinus-surgery-what-patients-should-know

Why These Problems Often Show Up Together
A deviated septum and chronic rhinosinusitis are different problems, but they often overlap. A septal deviation can narrow nasal passages, change airflow, and make it harder to deliver sprays/rinses effectively. Meanwhile, chronic sinus inflammation may persist even if nasal breathing improves.
Another practical issue: if the septum is very crooked, it can make it more difficult for the surgeon to see and reach the sinus drainage pathways during endoscopic surgery. That overlap is one reason ENTs sometimes recommend treating both in one session.
—
In short: septoplasty helps the airway; FESS helps the drainage—two complementary fixes for two distinct problems.
Symptoms That May Signal You Need Both Septoplasty and Sinus Surgery
Symptoms more suggestive of a deviated septum (structural blockage)
- Ongoing nasal obstruction, often worse on one side
- Trouble breathing through one nostril
- Congestion that doesn’t respond well to typical sprays/medications
- Frequent mouth breathing or waking with a dry mouth
A common patient example: “The left side always feels clogged, even when I’m not sick.”
Symptoms more suggestive of chronic rhinosinusitis (CRS)
- Facial pressure or fullness
- Thick drainage from the nose or down the throat (postnasal drip)
- Reduced sense of smell
- Recurrent sinus symptoms lasting 12 weeks or longer, which is a common threshold for chronic rhinosinusitis when supported by exam or imaging findings
- Headache that seems to track with congestion/pressure (note: many headaches blamed on the sinuses are actually migraines or another headache type)
If you want a deeper overview of long-lasting sinus symptoms, visit our chronic sinusitis resource: https://sleepandsinuscenters.com/chronic-sinusitis
The “combination” symptom pattern ENTs listen for
1) “I can’t breathe well through my nose,” and
2) “I keep dealing with sinus pressure, drainage, or repeated symptoms—despite treatment.”
When those themes show up together, ENTs often evaluate for both an anatomic blockage and ongoing sinus disease—because each problem can maintain the other.
—
If airflow is limited and sinus symptoms persist, your ENT may evaluate both structure and inflammation together.
Common Causes & Risk Factors (Patient-Friendly)
What causes a deviated septum?
- Being born with a septum that’s naturally off-center
- Injury/trauma (sports, falls, accidents)
- Prior nasal surgery (in some cases)
Some people don’t realize their septum is deviated until adulthood, when congestion or sleep disruption makes the asymmetry more noticeable.
What causes chronic rhinosinusitis (CRS)?
Chronic sinus problems are often multifactorial. Contributors may include:
- Allergies (allergic rhinitis)
- Nasal polyps
- Recurrent or persistent inflammation (sometimes with infection)
- Irritant exposure (smoke, pollutants)
- Anatomy variations that narrow drainage pathways
In other words, it’s rarely “one thing.” That’s also why the plan after surgery may still include medical therapy for inflammation control.
—
CRS is usually a mix of anatomy and inflammation—often requiring both medical and, when needed, surgical care.
First-Line (Non-Surgical) Treatments ENTs Usually Try Before Surgery
Many people assume surgery is the first step. In reality, ENTs often start with a structured non-surgical plan—especially for chronic sinus symptoms—because inflammation sometimes improves without an operation. Surgery is typically considered when symptoms and objective findings remain consistent with chronic rhinosinusitis despite appropriate treatment.
Medications and nasal care for chronic sinus symptoms
Depending on symptoms and findings, treatment may include:
- Saline irrigation/rinses
- Intranasal steroid sprays (technique and consistency matter)
- Allergy management (avoidance strategies, medications, testing, immunotherapy when appropriate)
- Antibiotics are used only when a bacterial infection is suspected or confirmed
A clinician might phrase it like: “Before we operate, we want to make sure we’ve treated the inflammation that can respond to medication.”
When “maximal medical therapy” isn’t enough
Surgery discussions usually happen when symptoms and quality-of-life impact persist despite appropriate therapy—and when nasal endoscopy/CT findings show ongoing blockage that aligns with the symptom pattern.
This alignment matters: ENTs avoid operating on CT findings alone if symptoms don’t line up, and they also avoid dismissing symptoms when imaging and endoscopy clearly show persistent disease.
—
Most patients try focused medical therapy first; surgery is considered when symptoms and findings persist together.
When ENT Specialists Recommend Combining Septoplasty + FESS
The most common scenario: deviated septum + chronic rhinosinusitis
A classic reason for septoplasty and sinus surgery in a single session is a patient who has:
- A septal deviation that significantly limits airflow and/or contributes to obstruction, and
- Chronic sinus disease that benefits from opening targeted drainage pathways
In these cases, septoplasty addresses the “hallway” (nasal passage), while FESS addresses the “rooms” (sinus drainage pathways). Another analogy patients find helpful: septoplasty helps the “front door” open normally, and FESS helps the “drains” work the way they’re supposed to.
Why doing them together can be more efficient for patients
When appropriate, a combined plan can offer practical advantages:
- One anesthesia event rather than two (a single operative session)
- One recovery period instead of separate septoplasty and sinus surgery recovery periods
- Often fewer total days of disrupted sleep, work, school, and exercise across the year
- Streamlined post-op follow-up planning
Research comparing combined surgery to septoplasty alone suggests that combined approaches can be performed safely without higher complication rates in selected groups, and that sinus surgery can improve disease-specific quality-of-life measures. [1–3]

Surgical sequence matters—why septoplasty is typically done first
In combined cases, ENTs commonly perform septoplasty first to straighten the septum and improve access/visibility for the sinus portion of the procedure. Better access can support more precise work around the sinus openings and help the surgeon address the areas identified on endoscopy and CT imaging. [4]
—
Treat the hallway first, then the rooms—so the surgeon can work precisely and safely where it matters most.

Is It Safe to Combine Septoplasty and Sinus Surgery?
What research shows about safety and complication risk
For many patients, published evidence suggests that combined septoplasty and FESS is generally safe and not associated with increased complication rates compared with septoplasty alone in studied groups. [1–2]
Potential risks (honest but not alarming)
All surgery has risks, and your ENT will review what applies to your situation. Commonly discussed considerations include:
- Bleeding
- Infection
- Scarring/adhesions
- Temporary (and sometimes persistent) congestion during healing
- Risks related to anesthesia and individual health history
- Less common risks specific to sinus surgery (reviewed during consent)
It’s normal to feel more congested early on—many patients say the first week feels like a “stuffy cold,” then improves in stages.
Who may not be a good candidate for combined surgery (examples)
A combined approach may not be ideal if:
- Medical conditions aren’t well controlled (making anesthesia or healing more complex)
- The sinus disease is unusually complex and a staged approach is preferred
- The septal deviation is mild and doesn’t affect breathing or surgical access
- A patient’s priorities favor addressing the most limiting problem first
In these scenarios, an ENT might recommend a more stepwise plan to keep risks low and goals clear.
—
For the right patient, combined surgery can be efficient and safe; for others, a staged plan may be the wiser path.
What to Expect Before Surgery (Evaluation & Planning)
ENT exam and nasal endoscopy
A typical evaluation may include an in-office exam and nasal endoscopy to assess:
- Septal deviation and overall nasal anatomy
- Turbinate size
- Mucus, swelling, and signs of inflammation
- Polyps (when present)
Endoscopy also helps the ENT distinguish between structural obstruction and swelling-driven congestion—which can guide whether septoplasty, sinus surgery, or both makes sense.
CT scan of the sinuses (when it’s used)
A sinus CT can help confirm chronic rhinosinusitis and identify which sinuses are blocked. It also helps the ENT plan a targeted procedure rather than a one-size-fits-all approach.
Questions to ask at your consult
Consider bringing these to your visit:
- “Which symptoms should improve from septoplasty vs. FESS?”
- “If I have allergies, what’s the plan after surgery?”
- “Will I have nasal splints or packing?”
- “How many follow-ups are typical after combined surgery?”
- “What should I expect for congestion and activity limits?”
If you work a physically demanding job, it’s also reasonable to ask: “When can I safely lift, bend, or return to workouts?”
—
A focused exam plus clear questions helps tailor the plan to your goals and anatomy.
What Recovery Looks Like (Combined Procedure Timeline)
Recovery varies by patient and by the extent of work performed, but these general milestones are common when septoplasty and sinus surgery are combined.
The first week
- Congestion is common, and breathing can feel worse before it feels better
- Saline rinses and any prescribed medications are central to early healing
- Sleep may be more comfortable with head elevation (when recommended)
Many patients also notice mild fatigue. Planning a lighter schedule—especially for the first several days—can make recovery feel more manageable.
Weeks 2–6
- Gradual improvement in airflow and sinus drainage as swelling decreases
- Follow-up visits are important; some patients may have gentle in-office cleaning/debridement if their surgeon recommends it
It’s common for improvements to be “two steps forward, one step back,” especially if you’re exposed to allergens or return to strenuous activity too quickly.
When patients often notice meaningful improvement
Many patients notice stepwise improvements rather than an overnight change. In research on endoscopic sinus surgery outcomes, quality-of-life improvements are commonly reported as healing progresses. [3]
—
Expect gradual, stepwise gains—consistent rinses and follow-ups help lock in results.

Lifestyle Tips to Support Healing and Long-Term Results
Do’s
- Use saline rinses exactly as directed
- Stay hydrated
- Attend follow-ups (especially important after sinus surgery)
- Follow activity guidance to reduce bleeding/swelling risk
A helpful mindset is “protect the healing tissues now to get the best long-term airflow and drainage later.”
Don’ts (common pitfalls)
- Smoke or vape (can worsen inflammation and slow healing)
- Overuse decongestant sprays (rebound congestion can occur)
- Return to strenuous workouts too soon
If you’re unsure what counts as “strenuous,” ask your surgeon for a clear timeline based on your specific procedure.
Long-term prevention strategy (especially for CRS)
Even after surgery, many patients do best with ongoing inflammation control, such as:
- Allergy management and irritant reduction
- Nasal steroid therapy if prescribed
- Addressing contributing factors like reflux when relevant
Surgery can improve airflow and drainage, but long-term comfort often comes from pairing that structural improvement with ongoing inflammation care.
—
Good daily habits plus targeted medical therapy help sustain your surgical gains over time.
Treatment Alternatives (When You Might Not Need Both)
Septoplasty alone
If symptoms are mainly airflow-related and sinus disease is minimal, septoplasty alone may be enough to address nasal obstruction.
FESS alone
If the septal deviation is mild and doesn’t limit breathing or access, an ENT may recommend sinus surgery without septoplasty.
Balloon-based sinus procedures (selected patients)
Some patients with specific anatomy and disease patterns may be candidates for balloon-based approaches. Whether that’s appropriate depends on imaging findings, symptom history, and endoscopic exam.
—
The “right” procedure is the least invasive option that reliably addresses your specific problems.
FAQs
Can a deviated septum cause sinus infections?
A deviated septum can contribute to obstruction and airflow issues, which may play a role in symptoms. However, nasal obstruction and sinus symptom patterns are often multifactorial—anatomy, inflammation, allergies, and other factors can contribute.
Why do ENTs do septoplasty first when combining surgeries?
Septoplasty is typically performed first to straighten the septum and improve access and visibility for the sinus portion of the procedure. [4]
Is combining septoplasty and FESS riskier than doing septoplasty alone?
In published comparisons, combined septoplasty and FESS has generally not shown higher complication rates than septoplasty alone in studied groups. [1–2]
Will this be one surgery or two?
When combined, it’s usually one operative session. Some situations may still call for staging, depending on anatomy, severity, and patient factors.
How long will I be out of work?
It depends on the extent of surgery and your job demands. Many people return sooner to sedentary work than to physically demanding work. Your ENT can give guidance tailored to your situation.
Will septoplasty change the outside shape of my nose?
Septoplasty is intended to correct internal nasal structure, and noticeable external cosmetic change is not usually expected. If you have concerns about appearance or prior trauma, bring that up during your consultation.
What if I still have symptoms after surgery?
Persistent symptoms can happen and don’t automatically mean surgery “failed.” Common reasons include ongoing allergies, chronic inflammation, polyps, migraine rather than sinus headache, reflux, or environmental irritants. Follow-up evaluation helps identify next steps.
—
Your care team can help troubleshoot lingering symptoms and fine-tune long-term management.
Conclusion + Call to Action
If you’re dealing with both persistent nasal blockage and chronic sinus symptoms, septoplasty and sinus surgery combined can be a safe, efficient approach for the right candidate—often improving breathing and sinus-related quality of life while minimizing the inconvenience of separate procedures. [1–3]
To review your symptoms, imaging, and options with an ENT, you can request an appointment with Sleep and Sinus Centers of Georgia: https://sleepandsinuscenters.com/appointments. If you’re ready, book a visit so your clinician can confirm whether septoplasty, FESS, or a combined approach best matches your goals.
—
The best plan is personalized—an ENT evaluation can clarify whether a combined approach is right for you.
Citations
1. Koch T, et al. (2016). Safety/effectiveness findings for combined septoplasty and endoscopic sinus surgery. PubMed (PMID: 26645244). https://pubmed.ncbi.nlm.nih.gov/26645244/
2. Bulut OC, et al. (2024). Outcomes/complications for combined septoplasty and sinus surgery. PubMed (PMID: 37706653). https://pubmed.ncbi.nlm.nih.gov/37706653/
3. Murrell GL, et al. (2011). Endoscopic sinus surgery outcomes and quality-of-life considerations. PMC3335522. https://pmc.ncbi.nlm.nih.gov/articles/PMC3335522/
4. American Academy of Otolaryngology–Head and Neck Surgery (AAO-HNS). Patient information on endoscopic sinus surgery. https://www.enthealth.org/conditions/endoscopic-sinus-surgery/
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
Don’t let allergies slow you down. Schedule a comprehensive ENT and allergy evaluation at Sleep and Sinus Centers of Georgia. We’re here to find your triggers and guide you toward lasting relief.